Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
The role of lung transplantation is to provide survival and quality of life benefits to patients with advanced lung disease. In this chapter, focusing on chronic obstructive pulmonary disease (COPD), we provide a comprehensive discussion of key aspects involved in the assessment of recipient suitability for transplantation. We discuss key issues such as timing of referral, donor evaluation, and organ allocation. We provide a detailed evaluation of the technical aspects of transplant surgery, evaluating the relative merits of both single and bilateral lung transplantation. In addition, we highlight how the transplant field is addressing donor shortfall, with expansion of acceptable donor criteria and the use of ex vivo lung perfusion to improve donor evaluation. Finally, we examine post-operative morbidity and mortality, discussing both early and late surgical complications and the adverse effects of long-term immunosuppression.
Beacon Hospital Dublin, University College Dublin, Ireland
Peter Riddell
Mater Misericordiae University Hospital, Dublin, Ireland
Diana Parau
Carol Davila University of Medicine, Romania
Alexandru Mihai Cornea
Mater Misericordiae University Hospital, Dublin, Ireland
*Address all correspondence to: allcornea@yahoo.com
1. Introduction
Lung transplantation (LTx) is a surgical intervention that aims to provide survival and quality of life (QoL) benefits to patients with advanced lung disease. However, this intervention is associated with significant peri-operative and long-term adverse risks. Identifying suitable candidates therefore requires a detailed evaluation of recipient risk factors by a multi-disciplinary team.
Chronic obstructive pulmonary disease (COPD) is one of the most frequent indications for LTx, accounting for approximately one-third of cases worldwide [1]. However, despite the high symptom burden as lung function declines, identifying patients who will achieve a survival benefit from LTx is not always straightforward. Multimodal assessment of lung function, exercise tolerance, and symptom burden (e.g. the BODE index) provides a good reference point for referral for transplant. However, additional factors that increase mortality risk from COPD, such as the development of pulmonary hypertension or chronic hypercapnia may influence listing decisions.
As an alternative to LTx, either as a temporizing intervention or for patients unsuitable for LTx, lung volume reduction techniques (surgical or bronchoscopic) may also be considered. However, these techniques also require specific eligibility criteria to be met, such as upper lobe predominant disease, so are not suitable for all patients. In selected cohorts, however, lung volume reduction can result in significant improvement in quality of life and exercise levels.
2. Transplant as a therapeutic option for emphysema in COPD patients
2.1 COPD as a progressive condition
The pathogenesis of COPD is characterized by chronic airway inflammation, resulting in fixed airflow limitation and alveolar wall destruction. Prolonged exposure to cigarette smoke is the key risk factor [2], but environmental exposures (vapors, dust, and workplace pollutants) have also been associated with the pathogenesis of this condition. Genetic risk factors, in particular alpha-1 antitrypsin (A1AT) deficiency, are also of importance [3]. Smoking also has the potential to affect other comorbidities that progress in tandem with COPD and can negatively impact functional status, survival, and fitness for transplant surgery.
2.2 Epidemiology of COPD
The natural history of COPD is characterized by increasing morbidity over time, which leads to increasing disability, respiratory failure, and eventually death. Transplantation therefore has the potential to confer quality of life and survival benefits to this cohort of patients. However, due to the risks involved, it is typically pursued only after all other treatment modalities have been exhausted.
COPD is highly prevalent. The WHO recognizes this condition as the third highest cause of mortality worldwide [4]. Given such a large denominator, it is apparent that only a very small percentage of COPD patients benefit from transplantation. The implementation of lung transplants is therefore highly specialized and is reserved for highly selected cases, where survival and QoL benefits are likely to be achieved. It is best considered within the setting of a specialist tertiary or quaternary center that operates in a hub-and-spoke service model to ensure equitable and geographically diverse access within a unified healthcare system.
2.3 Subtypes of COPD
A1AT deficiency is caused by a single gene abnormality, prevalent in certain populations [5]. A1AT inhibits elastase that when activated unopposed causes enzymatic destruction of host tissue. An imbalance in protease:anti-protease activity due to the functional reduction or absence of A1AT predisposing to development lung (COPD and bronchiectasis) and liver disease [6]. These observations were for many years the foundation of the elastase/anti-elastase pathogenesis hypothesis of COPD [7]. Diagnosis and family screening are crucial to identify patients with early or progressive disease [8]. Smoking cessation or, more importantly, avoidance is therefore the most significant treatment intervention [9].
Patients with A1AT deficiency who present with emphysema tend to do so at a younger age with fewer comorbidities and less functional impairment. Transplant registries tend to overrepresent A1AT deficiency among their emphysema cohorts due to these differences in clinical presentation, comorbid burden, and age [10]. Patients with A1AT deficiency as the defining reason for enrollment in a lung transplant program tend to have better outcomes [11]. For patients with A1AT deficiency who have developed concomitant lung and liver disease, multi-organ transplant may be necessary, but requires careful co-management in a center of excellence, to optimize the timing of transplantation and the quality of patient [12].
2.4 Survival in COPD
Predicting survival in COPD can be challenging, as disease progression does not follow a linear trend [13]. The BODE index is a tool that assists clinics with disease prognostication [14]. This simple clinical index considers airway obstruction measured by spirometry, physical features such as body mass index, exercise capacity measured using a six-minute walk test, and symptom score measured using the modified Medical Research Council dyspnoea scale. However, as the score was not originally developed to assess surgical patients, it may overestimate mortality risk in younger patients [15]. Modification using data from transplant registries may refine this index in surgical candidates in the future.
2.5 Comorbidities in COPD
COPD may be considered a multisystem disease not just limited to the lung. Smoking-related diseases of other organs can impede progression to transplantation. For example, atherosclerotic disease prevalence increases with cigarette smoking and advancing age. Atherosclerosis is frequent in those with emphysema, and studies have identified emphysema as an independent risk factor for coronary artery disease with a bi-directional relationship [16].
Coronary artery disease is frequently concordant with sclerosis of other vascular beds such as those of the cerebral circulation. As such, the identification and optimization of coronary artery and established vascular disease are prerequisites for patient selection and acceptance into a transplant program.
A host of other comorbidities are associated with COPD including metabolic syndrome, osteoporosis, sarcopenia, and malignancy [17]. These require identification and management and can have a variable impact on selection and management of lung transplant. They also increase the overall recipient risk profile as many of the symptoms are exacerbated by post-transplant immunosuppression. The complex permutations, combinations, and interplay of disparate pathophysiological processes create a heterogeneous patient population underscoring the importance of comprehensive and multi-disciplinary management.
2.6 Surgical management of COPD
The choice of the transplant procedure depends on various factors, including whether it involves a single lung, bilateral lung, or multi-organ transplant [18]. Multi-organ transplants may occur in tandem or sequentially, depending on clinical need. Lung transplant is not the only potential surgical intervention for patients with COPD; lung volume reduction surgery and other interventional therapies, such as endobronchial coils and valves, also have a role to play [19]. These enhanced surgical techniques may be part of or ancillary to a lung transplant program. Therefore, a patient may be referred for general surgical consideration, with lung transplant being one option among several considered by the thoracic transplant team.
In certain circumstances, lung transplant may follow other surgical approaches that act as a temporary measure or a bridge to transplant. Transplant surgery may be deferred, while patient care and performance status are optimized. The management of patients who have undergone prior surgical procedures may require additional consideration by the transplant team [20].
2.7 Prognosis and transplant
Patient selection for lung transplantation is based on a detailed assessment of a potential candidate’s individual risk profile. This assessment should involve a multi-disciplinary team of sub-specialty experts that includes transplant anaesthesiology, surgery, critical care, and pulmonology. The overriding principle of this decision-making process is to decide whether lung transplantation (assuming adequate allograft function) will be associated will survival and QoL benefits that are greater than medical management alone (i.e. no transplant).
This paradigm dictates that the morbidity and mortality associated with the intervention should be offset by the expected survival gain from treatment using a balanced risk-benefit assessment approach [21]. Conversely, the prognosis of the patient being selected for surgery should be significantly grave to achieve a survival advantage offered by the procedure. Paradoxically a poor short-term prognosis is often correlated with worsening performance status, making patients less suitable for surgery than their longer-lived counterparts.
2.8 Principles of patient selection
Given the scarcity of lung transplant as a life-saving treatment option, fairness and equity of access are particularly important and subject to justifiable societal scrutiny. An international consortium of the International Society for Heart and Lung Transplantation (ISHLT) provides consensus documents to facilitate the selection of patients by presenting appropriate, clinically based criteria. The current document [22], suggests that adults with chronic end-stage lung disease should have a two-year survival of less than 50 percent in the absence of transplant and a greater than 80 percent expected survival at 5 years, assuming adequate graft function post-treatment. Absolute contraindications have been emphasized in earlier documents [23] while relative contraindications may be tackled in centers with expertise in dealing with those specific contraindications.
2.9 Relative contraindications for lung transplantation
Advancing recipient age at the time of lung transplantation has been reported to adversely impact five-year survival [24]. Arbitrarily age-related cut-offs are avoided by most transplant programs, focusing instead on a potential recipient’s overall fitness — biological rather than chronological age — for transplant. However, in view of age-related-adverse risk, the 2021 ISHLT consensus statement describes an age between 65 and 70 years to be associated with unfavorable short and/or long-term outcomes. Furthermore, an age greater than 70 years at transplant is associated with substantially increased adverse risk [25].
Obesity also increases short-term and long-term post-operative complications and should be optimized as part of a pre-operative management algorithm [26]. Low body mass index also confers a similar risk. Nicotine dependence, identified through screening, requires explicit medical advice regarding abstinence. Tobacco abstinence can be confirmed using either cotinine or exhaled carbon monoxide measurement as part of a smoking cessation adherence program. Vaping of nicotine salts or products is harder to define and detect though also a concern [27]. A significant period of abstinence before surgery is a usual component of most programs. Despite the importance of this issue, ongoing tobacco abuse is surprisingly prevalent [28], with disappointing rates of cessation given the nature of the LT intervention.
2.10 Disease-specific triggers for transplant
A BODE score of greater than five is considered sufficient to initiate a referral for transplant assessment. Other factors to consider include the exacerbation phenotype of the patient, as frequent exacerbators have poor survival. More than one exacerbation per year represents a significant increase in short-term survival risk. Dynamic deterioration, such as an increasing BODE score by a unit of one in the previous 12 months, encourages referral. The ISHLT consensus recommends admission to a lung transplant waiting list for those with a BODE score in the range of 7–10, with an FEV-1 less than 20% of predicted and evidence of moderate rehabilitation potential [29]. Other factors associated with increased mortality risk, such as the development of pulmonary hypertension or hypercapnia, may also prompt transplant listing.
3. Recipient selection and listing criteria for LT for COPD
Performing a lung transplant for COPD presents significant challenges, with a path marked by numerous potential pitfalls and complexities. Determining the optimal timing for transplantation in these cases poses a challenge due to the prolonged stability observed in patients with consistent oxygen requirements. This timeframe is often referred to as the “transplant window”, representing the ideal period for offering an LT with the highest chance of success [30].
3.1 Referral for LT assessment
A patient with COPD is typically referred for LT when medical interventions have been exhausted and a decline in general health status has occurred. The 2021 ISHLT consensus statement on candidate selection, recommends referral for transplant assessment when the following criteria are met:
A BODE score of 5–6, in addition to one of the following:
Frequent acute exacerbations
Increase in BODE score > 1 point over 24 months
FEV1 20–25% predicted
Clinical deterioration despite maximal medical management
Quality of life that the patient considers to be unacceptably poor
3.2 Listing for LT
Patients typically meet specific listing criteria for COPD, characterized by advanced disease, usually at Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage IV [30].
In an otherwise suitable lung transplant candidate, achieving a BODE score of 7–10, associated with increased mortality risk, is recommended as the cut-off for transplant listing. Other factors, also associated with mortality risks, such as the presence of moderate-to-severe pulmonary hypertension, an FEV1, 20% predicted, a history of severe acute exacerbations, or the presence of chronic hypercapnia may also prompt listing, irrespective of BODE score [22].
Certain contraindications for LT are considered absolute, (see Table 1) such as the presence of high-grade malignancy (<5 years), acute medical instability due to acute myocardial ischemia, irreversible multi-organ failure, septic shock, severe coagulopathy, active substance abuse (alcohol, nicotine, marijuana, etc.), inadequate social support or nonadherence to medical therapy. Other risk factors are determinants for an increased chance of complications or unfavorable posttransplant outcome [22].
Absolute contraindications
Risk factors with high or substantially increased risk
Risk factors with unfavorable implications of posttransplant outcome
Candidates with these conditions are considered too high-risk to achieve successful outcomes post lung transplantation
Candidates with these conditions maybe considered in centers with expertise specific to the condition
While acceptable for lung transplant programs to consider patients with these risk factors, multiple risk factors together may increase the risk of adverse post-lung transplant outcomes
Factor or condition that significantly increases the risk of an adverse outcome post-transplant is most likely harmful for a recipient.
We may not have data to support transplanting patients with these risk factors or there is substantially increased risk based upon the currently available data, and further research is needed to better inform future recommendations.
Most lung transplant programs should not transplant patients with these risk factors except under very exceptional or extenuating circumstances.
When more than one of these risk factors is present, they are thought to be possibly multiplicative in terms of increasing risk of adverse outcomes. Modifiable conditions should be optimized when possible.
Lack of patient willingness or acceptance of Tx
Malignancy with high-risk of recurrence or death
Glomerular filtration<40 mL/min/1.73 m2, unless considered for multi-organ Tx
Acute coronary artery syndrome or myocardial infarction within 30 days
Stroke within 30 days
Liver cirrhosis with portal hypertension or synthetic dysfunction unless considered for multi-organ Tx
Other conditions (Acute liver failure, Septic shock, active tuberculosis, etc.)
Age over 70 years
Severe coronary artery disease requires coronary artery bypass grafting
Reduced left ventricular ejection fraction <40%
Sugnificant cerebrovascular disease
Severe esophageal dysmotility
Untreatable hematologic disorders including bleeding diathesis, thrombophilia, or severe bone marrow dysfunction.
Other factors as BMI > than or equal to 45 Kg/m2, Psychiatric conditions, Mycobacterium infections, etc.)
Age 65–70 years
Glomerular filtration rate 40–60 mL/min/1.73 m2
Mild to moderate coronary artery disease
Severe coronary artery disease that can be revascularized via percutaneous coronary intervention prior to transplant
Patient with prior coronary artery bypass grafting
Reduced left ejection fraction 40–50%
Other factors (peripheral vascular disease, connective tissue disorders, severe gastroesophageal reflux disease, etc.)
Currently, there is a shortage of available lung donors, resulting in a higher number of patients on waiting lists compared to the number of donors that are suitable for LT. However, there is a wide variation in donor acceptance rates across the world [31]. This may be associated with variability in healthcare models, prioritization of donor management in ICUs, and access to advanced assessment techniques, such as EVLP.
Ideal donor selection criteria are depicted in Table 2. The prevailing donor criteria are seldom met in contemporary settings, with only 15–25% of lung donors meeting these ideal criteria [33].
Ideal Donor selection criteria
Age < 55 years
No history of pulmonary disease
Normal serial chest radiograph
Normal gas exchange
Normal bronchoscopy
Size matching
Negative serologic screening for hepatitis B, and C and HIV
Consequently, ECDs have been devised to address these limitations. Commonly encountered extended donor lung criteria encompass anomalies in chest X-rays, a documented history of smoking, and marginal gas exchange levels. Lungs from donors more than 55 years old are now accepted for donation regularly [22]. Donors aged 60–70 are still considered eligible for donation despite evidence indicating that older ages have a higher 10-year mortality rate. The ECD also includes donors after pulmonary embolism or history of cancer or hypoxia-exposed lungs (less than 300 mm Hg which are now accepted for donation [33]. The use of lungs from donors with hepatitis B or C has been reported to be safe on both early and late treatment after lung transplantation [34]. The incorporation of the extended criteria has the potential to augment the donor pool by 50% [35].
In recent years, two additional approaches have emerged to address donor shortage; donation after cardiac death (DCD) and ex vivo lung perfusion (EVLP). EVLP, specifically serves as a technique for the functional assessment of lungs, determining their suitability for transplantation by evaluating their viability and usability [35].
The ideal lung donor selection criteria are summarized in Table 2 [32].
7.1 Brain-death heart-beating donors (DBD)
The predominant source of lung donations from transplantation comes from brain-dead heart-beating donors, largely due to widespread acceptance of brain death legislation across numerous countries. Japan stands out as an exception where the lack of legislation on DBD for many years spurred the development of living donor lung donations to boost the availability of lungs for transplant surgeries [36].
The assessment of donor lungs commences upon arrival at the donor hospital and involves multiple procedures. All pertinent information, including the donor’s medical history, cause of death, hospitalization detailed testing including ECGs, echocardiograms, chest X-rays, CT scans of the chest, ventilation support, medications administered (such as inotropes, diuretics, steroids), central venous pressures, arterial gas measurements, urine output, and pulmonary artery pressure, are carefully considered [36]. A checklist for donors can be employed to ensure that no details are overlooked see Table 3 [37].
Upon Arrival at the Procurement Center
Consent for donation
Verification of brain death that complies with local legislation if a DBD donor
ABO compatibility with the recipient
Serologies (Tissue types compatible for transplantation)
Supplies – tubing for preservation solution, preservation solutions, sternal saws, surgical equipment, bronchoscope, ice, saline, bags for organs, transport devices and organs
Any new information about the donor’s history since acceptance of any changes in the donor since acceptance to arrival at the procurement center
The evaluation process begins with bronchoscopy aimed at examining the bronchial anatomy for abnormalities, presence of secretions, foreign bodies, or other anomalies. Any secretions are cleared, and samples are collected for microbiological analysis through bronchoalveolar lavage. Any bronchial abnormalities or notable pathological findings, such as a lesion suspicious for malignancy, are promptly communicated to the transplant team. These factors may impact the decision regarding the acceptance of the lungs.
7.1.2 Intraoperative assessment of the lungs
The subsequent phase in evaluating a donor involves performing a median sternotomy, which entails surgically exposing the heart and lungs by creating a sizable opening in both pleural spaces. The lungs undergo assessment through visual inspection and palpation to detect masses, bullae, and nodules, and to evaluate for edema, consolidations, or contusions. All identified nodules will have a biopsy to rule out malignancy [36]. Patients who are donors commonly exhibit basal atelectasis due to prolonged mechanical ventilation. To address this, recruitment maneuvers are employed, including lung inflations using a Valsalva technique (air pressure around 20–25 cm H2O) and gentle expansion of the atelectatic regions. Typically, pulmonary vein gas analysis from all veins is required at FIO2 100% and PEEP of 5–7. Visceral pleural injury is not usually accepted because of risk of lung deflation during transportation and air leak during the surgical implantation [39].
7.2 Donors after cardiocirculatory death (DCD)
Donation after circulatory death (DCD) has the potential to increase the pool of lungs available for transplantation. DCD donors are individuals whose organs are retrieved after cardiac arrest [39]. The established criteria for death involve permanent cessation of both respiration and ventilation [39]. The Maastricht classification identifies four types of DCD donors (I-IV), the first two categories are uncontrolled deaths (uDCD), and the last two are controlled death categories, (cDCD III and IV). See Table 4.
Category
Description
Condition
I
Dead on arrival “in the field”
uncontrolled
II
Unsuccessful resuscitation
uncontrolled
III
Anticipated circulatory arrest
controlled
IV
Circulatory arrest in a patient previously declared brain-dead
controlled
V
Euthanasia or Medical Assistance in Dying (MAID) in hospital
controlled
Table 4.
Donation after cardiac death: Maastricht categories [35].
Category III donors (cDCD) are preferred in DCD because the patient is in hospital and the process of withdrawal, cardiac arrest, and lung retrieval can be planned and controlled. The duration of warm ischemic time (WIT) for DCD donor lungs has been a subject of debate. Some authors consider that WIT starts when the BP < 50 mm Hg and ends with the onset of pulmonary artery flush [39]. The consensus among most centers is that lungs remain viable for LT within a window of 60 to 90 minutes after circulatory arrest [39]. Donor selection criteria for cDCD are like DBD and extended criteria; age > 65 years old, smoking history>20 packs/years, abnormal chest X-Ray, and can be applied to cDCD equally well. The unique aspect of DCD lung retrieval involves conducting bronchoscopy and obtaining arterial gas samples before donor’s death. The bronchoscopy can be done in the theater after the reintubation of the airway.
7.3 Living donor lobar lung transplantation (LDLLT)
LDLLT serves as a viable alternative to the traditional lung donation methods (from DBD or DCD donors), particularly in critical situations where a patient may not survive long enough to receive a lung from a DBD or DCD donor. Originally designed for pediatric cystic fibrosis patients, this procedure can now be employed for various conditions like restrictive, obstructive, infectious, or vascular lung disease. Due to its complexity, requiring two living donors, it is typically reserved for centers with expertise in this field [40, 41].
The surgical procedure involves two primary steps: preliminary dissection and lung cannulation, followed by lung harvesting. The objective of the preliminary dissection is to isolate essential anatomical structures, facilitating the seamless harvest and preservation of the lungs. The dissection initiates with the placements of pericardial stay sutures, followed by separation of superior vena cava from the pulmonary artery (PA). Subsequently, the dissection progresses involving the inferior vena cava (IVC), ligation of azygos vein (AV), and the separation of the aorta from PA [42]. Both pleurae are widely opened, and pulmonary ligaments are divided. Tracheal dissection is approached between aortic arch and SVC and can be done now or later when the lungs are harvested. Cannulation is done after a 4–0 Polypropylene purse-string suture is placed on the pulmonary artery trunk 1.5 cm proximal to the bifurcation and one more on the ascending aorta. Heparin is administered intravenously 400Units/kg. The cannulas are inserted in the PA and aorta and are connected to the lines and de-aired. The preservation solution (Perfadex) is prepared, and infusion tubes are primed. Prostaglandin E 250 ug is injected into the PA trunk. The SVC is tied and IVC is partially transected, and one pool-tip sucker is inserted into IVC to prevent warm blood from abdominal organ perfusion to reach the pericardium and pleural spaces. The left atrium (LA) appendage is cut to vent the left atrium and prevent heart distension. The surgical strategy for lung harvest differs if both heart and lungs are collected or only the lungs. If both heart and lungs are harvested best option is to open LAA and insert a pool-tip sucker into the LA. The Waterston interatrial groove is dissected, and LA is open, the heart apex is elevated, and an incision is made into LA between the pulmonary veins and coronary sinus anterior to the left pulmonary veins. Next, an aortic clamp is applied on the ascending aorta, and cardiac preservation solution is started followed by the lung preservation solution. In all this time the lungs will be ventilated with low tidal volumes at FIO2 100% [42]. The cold saline is slushed into the chest around the lungs and the heart. Some surgeons avoid using cold saline for lungs because of risk of injury. The next step is heart explanations which are performed by whole IVC transection, LA incision in Waterston’s groove, heart is lifted, and a second incision is made in LA between coronary sinus and left pulmonary veins. The right and left LA incisions are connected, and heart is lifted cephalad, and right and left atriotomies the rest of LA is cut on the superior part. Then the SVC is transected, the aorta is cut distally, and the PA is exposed and transected at bifurcation [43].
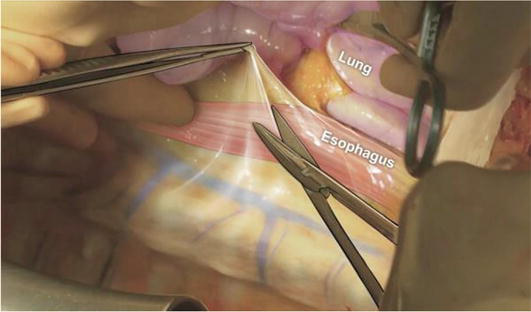
The excision of the lung block begins by releasing the pulmonary ligaments, making an incision in the posterior pericardium beyond the pulmonary veins to expose the esophagus (Figure 1).
Figure 1.
Dissection of the anterior margin of the esophagus on right and left side [15, 43]. This is an open access article, distributed under the terms of the creative commons attribution non-commercial license https://creativecommons.org/licenses/by-nc/4.0 which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The esophagus serves as a pivotal anatomical reference point for facilitating lung extraction [43]. Dissection on the right side continues on the anterior surface of the esophagus until reaching and dividing the azygos vein. Similarly, on the left side, dissection follows the esophagus and progresses until the aorta which is divided. Subsequently, the anterior exposure of the trachea involves dividing the innominate artery and preparing it circumferentially. With inflation of the lungs and a brief breath hold the trachea is stapled and divided. The lung block is removed from the chest and submerged in an ice solution. An additional retrograde perfusion of 1 liter Perfadex is administered through the pulmonary veins to flush any potential clots from the pulmonary arteries [43]. One the flushing process results in clear fluid the lungs are typically separated and placed in a sterile plastic bag filled with preservation solution. This bag, along with two more plastic bags filled with ice solution, is utilized to store the lungs in an ice cooler for transportation to the recipient hospital.
8.2 Lung procurement in DCD donors
Lung procurement in DCD is different from that of DBD donors and the main steps are described below. The procedure begins with a notification to the operating theater to be ready for DCD procurement. Subsequently, a pre-withdrawal meeting convenes, involving all relevant staff. This meeting serves to review the consent details and delineate responsibilities. The withdrawal takes place in either the ICU or the operating room, with inotropic support discontinued and extubation performed [38]. The process of controlled DCD (cDCD) lung retrieval starts with withdrawal from life support if the cardiac arrest occurs in 60–90-minutes intervals [42]. If the cardiac arrest happens, then death is caused by lack of pulsatility of arterial line with or without electrical activity [38] and heparin can be given at this stage (or before the cardiac arrest). There is a “no touch” period of usually 2–5 minutes. If the heparin was administered after death certified, 20 chest compressions are necessary for heparin to circulate in the body. The patient is moved to the operating theater where the surgical team is ready for surgery. The endotracheal tube either remains in place or is removed and the patient is reintubated in theater and a single breath is given until the perfusion solution is started and aorta is clamped to avoid cerebral perfusion resuscitation. [38, 42]. Median sternotomy is performed, and the pulmonary artery is cannulated, Prostaglandin E1 500 micrograms and Perfadex solution are perfused into the lungs (50–70 ml/kg) antegrade and retrograde. The bronchoscopy can be done at this stage by one of the surgeons or anesthesiologists. The left atrial appendage is open for draining the perfusion solution and the lungs are ventilated. The pleural spaces are open, cold saline is infused and the lungs are inspected. The heart is explanted, and the lungs are removed from the chest, with same technique as in DBD previously presented, retrograde flushing is performed packing and storage as in DBD, and are transported to the recipient hospital [42]. If the lungs are borderline, they will be removed en bloc (without separation) and sent to the main hospital for ex vivo perfusion (EVLP) to be assessed and repaired. The decision for LT will be delayed at the end of the EVLP [42].
8.3 Ex vivo lung perfusion (EVLP)
EVLP is a technique aimed at increasing the number of lung transplants by assessing and repairing borderline organs. To accomplish this the lungs are ventilated and perfused outside the body. It is well-known that lungs suffer many injuries during the harvesting time, because of warm ischemia secondarily to the type of donation (DCD or DBD) or because of the donor pathology itself, smoking, chest contusion, aspiration, pneumonia, etc. Ex vivo lung perfusion (EVLP) provides critical insights into lung function and can potentially address some deficiencies, ultimately rendering the organ suitable for transplantation. The rationale behind EVLP lies in the advantages of maintaining normal lung temperature, providing oxygen and nutrients, and allowing real-time assessment and rehabilitation of the lungs.
EVLP employs a centrifugal pump for perfusion and follows a lung protective strategy using low tidal volumes for ventilation. Various protocols exist for EVLP, the Toronto protocol being widely adopted due to its extensive experience [44]. The Toronto protocol involves using acellular perfusate, a closed circuit maintaining positive left atrial pressure, and a low perfusion flow. The process includes specific steps such as connecting the lung graft to the perfusion system, initiating perfusion with solution, and gradually warming the lungs while employing protective ventilation strategies. Throughout the EVLP procedure, assessment is conducted regularly, including arterial gas analysis, pressure measurements, compliance checks, and solution loss. Additionally, X-rays and bronchoscopies are performed. Upon completion, the lungs are cooled, prepared according to the standard preservation protocols, and if deemed suitable, are readied for transplantation in the operating suite. A recent study reaffirmed that when evaluating lung quality, compliance, and airway pressures carry greater significance than oxygenation capacity. There are no differences in CLAD between the LT post-EVLP group and non-EVLP LT [45].
There are two main procedures routinely used in COPD, Single Lung Transplantation (SLT) and Double Lung Transplantation (DLT). In special circumstances, living donor lobar lung transplantation (LDLLT) can be a solution for small chest recipients or children where the chance to get an adult donor of the same size is low. Choice of procedure. Single lung transplantation and double lung transplantation are both recommended in patients with severe COPD, but for A1AT DLT is the procedure recommended.
9.1 Single lung transplantation (SLT)-surgical technique
Single lung transplantation is a very useful procedure for end-stage COPD because technically easier, less time-consuming, and less blood loss and intraoperative complications.
9.1.1 Position
The patient is placed in a lateral decubitus or supine position for either postero-lateral or anterolateral thoracotomy. Preparations for ECMO involve marking the femoral artery pulsations on both sides of the inguinal areas. The airway is intubated with a left-sided double-lumen tube or single-lumen tube in smaller patients with a blocker to permit single lung ventilation. Typically, the routine requirements for lung transplantation include the use of an autologous blood recovery system like cell saver, along with a Swan Ganz catheter for monitoring pulmonary artery pressure. Additionally, a deep venous catheter is commonly inserted into a jugular vein [46].
9.1.2 Approach
The incision is usually in the fifth postero-lateral intercostal space or 4th intercostal space for anterolateral thoracotomy.
9.1.3 Pneumonectomy
At this point one-lung ventilation takes place, and cardiac assistance devices such as ECMO or cardiopulmonary bypass (CPB) are employed in the event of hypoxia or hemodynamic instability. If the patient has severe pulmonary hypertension is better to start cardiac assistance before one-lung ventilation [47]. The initial stage is pneumonectomy which begins by accessing the pleural space, releasing the adhesions between the lung and pleura. The electrocautery is used for cutting the adhesions and achieving hemostasis. Afterward, the pulmonary veins are dissected and separated using a stapler prior to the initial division, followed by the dissection and section of the pulmonary artery beyond the first lobar branch. Then the bronchus is transected before the origin of the upper lobe branch, facilitating the removal of the lung from the chest. The peri bronchial tissue may be preserved to avoid the risk of ischemic damage. Hemostasis can be attained by identifying and halting bleeding from bronchial arteries.
9.1.4 Hilar preparation
Following lung removal, the stumps of bronchus and pulmonary vessels are identified and meticulously dissected to enhance their length and mobility. The peri bronchial tissue undergoes careful dissection, with a partial preservation approach aimed to prevent bronchial ischemia. This method ensures that bleeding from bronchial arteries or mediastinal tissue can be promptly addressed before proceeding to the anastomosis.
9.1.5 Donor lung preparation
The donor lung preparation takes place on the back table after removal from the ice box and involves examining the pulmonary artery, pulmonary veins, and bronchus integrity and trimming out the excessive surrounding tissue. In cases where the atrial cuff is insufficiently long and lacks tissue around pulmonary veins, an autologous pericardium patch can be used for enlargement [47]. The size of pulmonary artery is meticulously assessed, and if it is found to be excessively long, adjustments are made to prevent kinking and thrombosis of the anastomosis. The assessment of lung size involves comparing the chest dimensions usually by total lung capacity (predicted and actual). If the lung is deemed excessively large, a reduction surgery on the back table may be considered [47], or if considered can be oversized on purpose. Subsequently, the bronchus is sectioned, the lung is deflated, and is introduced in the chest for implantation.
9.1.6 Lung implantation
The process of lung implantation initiates with bronchial anastomosis, followed by the connection of the pulmonary artery and the left atrial cuff, encompassing the pulmonary veins [46].
9.1.7 Bronchial anastomosis
Bronchial anastomosis is the first anastomosis and requires meticulous attention due to the elevated risk of complications associated with ischemia or technical errors. The bronchus length is carefully assessed and divided by a scalpel, approximately 1 cartilage before the secondary carina, ensuring it’s as short as feasible without raising the risk of dehiscence. Various techniques have been devised for bronchial anastomosis. The first technique involves a continuous running suture around the entire circumference using a 4/0 polydioxanone suture.
Another technique largely used employs a posterior running suture on the membranous part of the bronchus, completed by interrupted stitches on the anterior cartilaginous part (see Figure 2). This technique is used by most surgeons because gives less complications. If there is a mismatch between the bronchi a telescopic suture is used by taking smaller bites on the donor aiming to fit the donor bronchus into the recipient [48]. Afterward, an air leak test is performed, and the anastomosis integrity is checked by intraoperative bronchoscopy.
Figure 2.
Right bronchial anastomosis (A) First suture outside-in on recipient at membranous-cartilaginous part (B) Same suture inside-out in the donor bronchus [48]. Open access this article is licensed under a creative commons attribution 4.0 international license, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the creative commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s creative commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s creative commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
9.1.8 The pulmonary artery anastomosis
The arterial anastomosis is the second anastomosis and initiates with the application of a clamp at the proximal site of PA followed by the careful adjustment of the two arterial stumps. Typically, a continuous 5.0 polypropylene suture is used, starting at the posterior wall, and progressing to the anterior wall (see Figure 3). The clamp is left in place until the left atrial (LA) anastomosis is completed facilitating de-airing of the lung [46].
Figure 3.
(A) Right pulmonary artery anastomosis-Duval clamp and Babcock forceps to hold the PA stump. (B) Clamp is wrapped and fixed to the drape followed by artery opening and preparation for anastomosis [48]. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
9.1.9 Left atrial anastomosis
The final anastomosis, involving the left atrium (LA) commences with careful application of a Satinski clamp to ensure uninterrupted coronary artery flow and prevent hemodynamic instability. The recipient LA stump is incised, creating two openings that are subsequently joined to form a single anastomotic site. Both LA openings are meticulously readjusted by trimming the excess tissue, and the LA anastomosis is carried out using a single continuous non-resorbable polypropylene 4.0 suture [46]. Some surgeons opt for an everting technique, to prevent muscular tissue from reaching the LA cavity and increasing the thrombotic risk (Figure 4).
Figure 4.
See the intima-to-intima suture of LA anastomosis. The left atrial anastomosis posterior wall suture between donor and recipient LA [48]. Open access this article is licensed under a creative commons attribution 4.0 international license, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the creative commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s creative commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s creative commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
9.1.10 Lung reperfusion
The lung reperfusion goal is de-airing the lung vasculature to avoid brain and coronary artery embolism. Two methods are available: retrograde flush or antegrade flush, both of which should be completed to achieve optimal results. The retrograde flush involves opening the atrial clamp while keeping the arterial clamp in place coupled with gentle lung ventilation. Conversely, the antegrade flush begins by slowly releasing the pulmonary artery (PA) clamp, keeping the left atrium (LA) clamp closed, and ultimately releasing the atrial clamp [46].
9.1.11 Thoracotomy closure
Following lung implantation and reperfusion, two pleural drains are inserted, and the thoracotomy is closed in anatomical layers. In cases where the sternum was cut to improve exposure during the procedure, the sternal edges will be reapproximated using sternal wires [46].
Usually, the patient is in supine position, and the chest, abdomen, and legs are prepared for surgery. The site of both femoral arteries is identified and pointed by a marking pen. The most used incision for double lung transplantation (DLT) involves a bilateral anterolateral thoracotomy combined with sternotomy (clamshell incision). This approach offers the best exposure for both lungs and facilities access to the pericardium, especially when using veno- arterial extracorporeal membrane oxygenation (ECMO). Alternatively, bilateral anterolateral thoracotomies without sternal cuts can be used to avoid sternal involvement. However, this method provides less exposure. In rare cases requiring cardiopulmonary bypass, median sternotomy can be utilized. DLT involves sequential explanting and implanting of the new lungs, starting with the more severely affected lung and then proceeding to the other. Anesthesia uses a double-lumen ventilation endotracheal tube for selective ventilation, along with transesophageal echocardiography and intraoperative bronchoscopy during surgery. Following the clamshell incision, and sternal cut specific attention is paid to dividing both internal mammary arteries, and then the pleural cavity is opened. The surgery progresses with the explant of the first lung by separating pleural adhesions and division of the inferior pulmonary ligament. Preservation of the phrenic nerve may be considered. Tapes are used to encircle the pulmonary veins and arteries, which are then cut by stapler. The bronchus is subsequently divided with a scalpel, and meticulous hemostasis of the bronchial arteries is necessary to prevent bleeding which becomes difficult to control once the new lung is in situ [35]. The implanting of the first lung uses the techniques described in SLT surgical procedure. The lung more severely affected by disease is prioritized for transplantation. Once the first lung is implanted, it is reperfused and the decision to use the Extracorporeal Membrane Oxygenation (ECMO) or CPB depends on any alterations in hemodynamics or oxygenation. Some experts advocate for routine CPB usage in DLT to prevent overperfusion of one lung during the implantation of the second, which can elevate the risk of post-transplantation Graft Dysfunction (PGD). Recent years have seen successful utilization of ECMO in these scenarios, offering a lower risk of bleeding compared with CPB, a reduced systemic inflammatory response, and a low transfusion rate [35, 47]. The implantation process for the second lung follows a similar protocol, commencing with pneumonectomy. Subsequently, the lung is implanted, and a bronchoscopy is conducted to verify the patency of the bronchial tree.
9.3 Living donor lung transplantation (LDLLT)
LDLLT consists of a right lower lobectomy from right-side donor, a left lower lobectomy from a left-side donor, and bilateral lobar implantation for the recipient [49]. The procedure is very complex and is recommended to be done in centers with experience in the field. It addresses very sick patients cohort which have no time to wait for a DBD or DCD donor. Size matching is very important as only two lobes are implanted and both functional and anatomical matching are used for evaluation. The procedure needs three operating rooms and four surgical teams, for right-side donor, left-side donor, back table team, and recipient team. The LDLLT is done with ECMO or Cardiopulmonary bypass (CPB). The main steps of the procedure are clamshell incision with sternal division, followed by ECMO placement, right pneumonectomy, right graft implantation and reperfusion, left pneumonectomy followed by left graft implantation and reperfusion, weaning the ECMO, and chest closure. After harvesting the lobes are flushed with a preservation solution before implantation [49].
10. Early surgical complications after lung transplantation
Primary surgical complications following lung transplantation can be categorized into airway, vascular, and additional complications, such as pleural, size mismatch, phrenic nerve palsy, or wound-related problems. Primary graft dysfunction frequently occurs following LT, while other complications such as acute and chronic allograft rejection are not referred to in the present chapter.
10.1 Airway complications
Arise because of bronchial ischemia, attributed to the division of bronchial arteries responsible for vascularizing the bronchus, the blood supply is assured by retrograde flow from the pulmonary artery. This encompasses conditions such as ischemia, necrosis, stenosis, dehiscence, and malacia [50]. Typically, necrosis either resolves spontaneously or progresses to dehiscence, which can be addressed through stent implantation. In severe instances, surgical repair becomes imperative. Following re-anastomosis vascularized flaps from intercostal muscle, or omentum can be employed to facilitate recovery. Stenosis is a common complication that often requires balloon dilatation or argon plasma therapy for resolution [50].
10.2 Vascular complications
Primary vascular complications are bleeding, stenosis of the anastomosis, thrombosis of PA or pulmonary veins, and kinking. Bleeding at the anastomosis usually requires reinforcement, although this may elevate the risk of stenosis. If the bleeding proves uncontrollable, it may be necessary to redo the anastomosis. Kinking occurs when the two arterial stumps are excessively long, potentially leading to thrombosis (Figure 5).
Figure 5.
Left pulmonary artery anastomotic occlusion post-lung transplantation [51]. The author(s).2019 open access this article is distributed under the terms of the creative common international license (https://creativecommons.org/license/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the creative commons license, and indicate if changes are made.
Treatment typically involves anticoagulation and insertion of a stent. Pleural complications are effusion, pneumothorax, empyema or chylothorax. Post-lung transplantation pneumothorax is a relatively common occurrence attributed to lung mismatch, air leak resulting from bronchial anastomotic dehiscence, or parenchymal issues. Typically, resolution is achieved through the appropriate management of chest drains [51].
10.3 Primary graft dysfunction (PGD)
PGD stands out as a prevalent cause of early morbidity in lung transplantation, with an incidence of 30% [50]. It manifests through hypoxia and radiologic opacities within the initial 72 hours following surgery (Figure 6). Bronchoscopy is used in these cases to evaluate the bronchial anastomosis and to obtain samples for microbiology [51].
Figure 6.
Primary graft dysfunction [51]. Axial CT images show smooth interlobular septal thickening with ground-glass opacities in the transplanted left lung [22]. The author(s).2019 open access this article is distributed under the terms of the creative common international license (https://creativecommons.org/license/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the creative commons license, and indicate if changes are made primary graft dysfunction: Imaging and transbronchial biopsy findings. Axial CT images show smooth interlobular thickening with ground-glass opacities in the transplanted left lung.
10.4 Other complications
Encompasses wound dehiscence, diaphragmatic palsy, or heart compression leading to pulmonary edema, particularly in double lung transplantation with oversized lungs. Addressing the latter complication may require temporary maintenance of an open chest cavity.
11. Early and long-term outcomes in lung transplantation for COPD
The success of lung transplantation (LT) for chronic obstructive pulmonary disease (COPD) is highly dependent on timing of the procedure. Optimal timing is critical, as undergoing LT too early may decrease survival rates, while waiting too long can lead to an increased mortality rate on the waiting list. While age itself does not impose a limitation on LT, it’s noteworthy that there is a 20% increase in patients aged over 60. However, advancing age may introduce additional comorbidities, potentially contributing to a decrease in 10-year survival rates [33]. The extended donor lung criteria have demonstrated that including heavy smokers as donors does not adversely impact long-term survival. Moreover, individuals positive for hepatitis B and C can be considered viable donors for lung transplantation. In some cases, nonmelanoma skin cancer donors may not pose a significant barrier to lung transplantation and LT might be possible in pulmonary embolism if emboli are well-managed [33]. The utilization of controlled deceased circulatory death donors (cDCD) has led to a donation rate surge of 20–50% in certain countries, whether employing ex vivo lung perfusion (EVLP) or not. Effective utilization of EVLP proved advantageous for assessing and repairing lungs, enabling a secure extension of preservation time by over 12 hours without adversely impacting long-term survival.
The A1AT cohort demonstrated a superior median survival compared to the COPD cohort (6.4 vs. 5.5 years) [52]. However, it’s worth noting that the A1AT cohort had a younger age at the time of transplant (51.9 vs. 59.7), which may explain the improved survival. In terms of long-term survival, the A1AT cohort exhibited a 43% survival rate, while the COPD cohort showed a lower survival rate of 23% [52]. In the initial year post-LT, the primary causes of death were infection and graft failure. However, in the long term, chronic lung allograft dysfunction (CLAD) emerged as the predominant cause of mortality [53]. Concerning double-lung transplantation (DLT) versus single lung transplantation (SLT), COPD stands out as the primary indication for SLT, with no observed enhancement in long-term survival for DLT [53]. When comparing lung transplantation in controlled donation after circulatory death (DCD) with donation after brain death (DBD), the one-year survival rates were 97 versus 90%, and at 5-year mark, the rates were 90 versus 61% [38]. Long-term survival rates for living donor lobar lung transplantation (LDLLT) in centers with extensive expertise in the field are 80% at 5 years, 72.6% at 10 years, and 61.7% at 15 years [54]. According to Verleden et al. [55] after the ISHLT report, the one-year survival post-lung transplantation (LT) is reported at 87%. The overall 5-year survival rate is 71%, with DLT exhibiting a more favorable outcome at 74% compared to 61% for SLT. Delving into 5-year mortality rates, chronic obstructive pulmonary disease (COPD) records 70.4%, while idiopathic pulmonary fibrosis (IPF) stands at 67%. Notably, the median survival for COPD and A1AT is significantly higher at 7.9 years, surpassing COPD without A1AT at 6.2 years [55]. In a study conducted by Gulack BC [56], examining 9569 patients of whom 14.6% were diagnosed with A1AT, unadjusted comparisons for SLT patients’ characteristics, revealed that individuals with A1AT tend to be younger and less prone to smoking, hypertension, or diabetes. When unadjusted outcomes were compared between A1AT and COPD, there were statistically significant findings indicating more airway dehiscence and higher likelihood of rejection in the A1AT group compared with COPD alone. The same author [56] in unadjusted comparisons involving DLT for A1AT, found a higher probability of recipients being younger and less likely to be female. Initial outcomes suggested a higher incidence of airway dehiscence and rejection compared to cases involving COPD only. Notably, the total hospital stay tended to be significantly shorter than COPD cohort.
12. Conclusions
Lung transplantation becomes necessary for COPD patients in advanced stages characterized by diminished quality of life, limited life expectancy, and the presence of difficult medical choices.
Evidence support the notion that single lung transplantation is not inferior to double-lung transplantation. Both procedures have now well-defined indications, with individuals with A1AT deficiency considered candidates for DLT and those with emphysema eligible for either SLT or DLT.
Technical factors play a crucial role in the choice between single-lung transplantation (SLT) and double-lung transplantation (DLT). SLT offers the benefit of shorter procedures and fewer intraoperative complications, whereas DLT tends to be longer with a higher likelihood of utilizing blood products or additional devices like ECMO, adding to the overall complexity. Studies have shown that early mortality rates are higher in DLT compared with SLT; however long-term survival, overall, is slightly better with DLT. DLT has another benefit as it can be employed in cases involving marginal donors, where utilizing a single lung is not practical, but employing two lungs is more suitable for ensuring optimal overall function [57]. Lung transplantation for emphysema poses a complexity due to the intricate task of matching the appropriate organ with the suitable recipient at the optimal time.
References
1.Son J, Shin C. Indications for lung transplantation and patient selection. Journal of Chest Surgery. 2022;55(4):255-264
2.Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. The Lancet. 2022;399(10342):2227-2242
3.Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: Risk factors, pathogenesis, and implications for prevention and treatment. The Lancet Respiratory Medicine. 2022;10(5):497-511
4.Safiri S, Carson-Chahhoud K, Noori M, Nejadghaderi SA, Sullman MJM, Heris JA, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: Results from the global burden of disease study 2019. BMJ. 2022;378:e069679
5.Carroll TP, O’Connor CA, Floyd O, McPartlin J, Kelleher DP, O’Brien G, et al. The prevalence of alpha-1 antitrypsin deficiency in Ireland. Respiratory Research. 2011;12(1):91
6.Lachaux A, Dumortier J. Hepatic involvement in hereditary alpha-1-antitrypsin deficiency. Revue des Maladies Respiratoires. 2014;31(4):357-364
7.Gooptu B, Ekeowa UI, Lomas DA. Mechanisms of emphysema in α1-antitrypsin deficiency: Molecular and cellular insights. The European Respiratory Journal. 2009;34(2):475-488
8.Hiller AM, Piitulainen E, Tanash H. The clinical course of severe Alpha-1-antitrypsin deficiency in patients identified by screening. International Journal of Chronic Obstructive Pulmonary Disease. 2022;17:43-52
9.Miravitlles M, Dirksen A, Ferrarotti I, Koblizek V, Lange P, Mahadeva R, et al. European Respiratory Society statement: Diagnosis and treatment of pulmonary disease in α(1)- antitrypsin deficiency. The European Respiratory Journal. 2017;50(5):1700610
10.Giacoboni D, Barrecheguren M, Esquinas C, Rodríguez E, Berastegui C, López-Meseguer M, et al. Characteristics of candidates for lung transplantation due to chronic obstructive pulmonary disease and alpha-1 antitrypsin deficiency emphysema. Archivos de Bronconeumología. 2015;51(8):379-383
11.Riley L, Lascano J. Clinical outcomes and survival following lung transplantation in patients with Alpha-1 antitrypsin deficiency. Respiratory Medicine. 2020;172:106145
12.Zamora MR, Ataya A. Lung and liver transplantation in patients with alpha-1 antitrypsin deficiency. Therapeutic Advances in Chronic Disease. 2021;12(Suppl.):20406223211002988
13.Young AL, Bragman FJS, Rangelov B, Han MK, Galbán CJ, Lynch DA, et al. Disease progression Modeling in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine. 2020;201(3):294-302
14.Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, et al. The body- mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. The New England Journal of Medicine. 2004;350(10):1005-1012
15.Pirard L, Marchand E. Reassessing the BODE score as a criterion for listing COPD patients for lung transplantation. International Journal of Chronic Obstructive Pulmonary Disease. 2018;13:3963-3970
16.Daher A, Dreher M. The bidirectional relationship between chronic obstructive pulmonary disease and coronary artery disease. Herz. 2020;45(2):110-117
17.Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. The European Respiratory Journal. 2009;33(5):1165-1185
18.Santambrogio L, Tarsia P, Mendogni P, Tosi D. Transplant options for end stage chronic obstructive pulmonary disease in the context of multidisciplinary treatments. Journal of Thoracic Disease. 2018;10(Suppl. 27):S3356-S3365
19.Ashraf O, Disilvio B, Young M, Ghosh S, Cheema T. Surgical interventions for COPD. Critical Care Nursing Quarterly. 2021;44(1):49-60
20.Slama A, Ceulemans LJ, Hedderich C, Boehm PM, Van Slambrouck J, Schwarz S, et al. Lung volume reduction followed by lung transplantation in emphysema-a Multicenter matched analysis. Transplant International: Official Journal of the European Society for Organ Transplantation. 2022;35:10048
21.Laupacis A, Sackett DL, Roberts RS. An assessment of clinically useful measures of the consequences of treatment. The New England Journal of Medicine. 1988;318(26):1728-1733
22.Leard LE, Holm AM, Valapour M, Glanville AR, Attawar S, Aversa M, et al. Consensus document for the selection of lung transplant candidates: An update from the international society for heart and lung transplantation. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation. 2021;40(11):1349-1379
23.Weill D, Benden C, Corris PA, Dark JH, Davis RD, Keshavjee S, et al. A consensus document for the selection of lung transplant candidates: 2014-an update from the pulmonary transplantation Council of the International Society for heart and lung transplantation. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation. 2015;34(1):1-15
24.Inci I, Schuurmans M, Ehrsam J, Schneiter D, Hillinger S, Jungraithmayr W, et al. Lung transplantation for emphysema: Impact of age on short- and long-term survival. European Journal of Cardio-thoracic Surgery: Official Journal of the European Association for Cardio-thoracic Surgery. 2015;48(6):906-909
25.Mosher CL, Weber JM, Frankel CW, Neely ML, Palmer SM. Risk factors for mortality in lung transplant recipients aged ≥65 years: A retrospective cohort study of 5,815 patients in the scientific registry of transplant recipients. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation. 2021;40(1):42-55
26.Upala S, Panichsillapakit T, Wijarnpreecha K, Jaruvongvanich V, Sanguankeo A. Underweight and obesity increase the risk of mortality after lung transplantation: A systematic review and meta-analysis. Transplant International: Official Journal of the European Society for Organ Transplantation. 2016;29(3):285-296
27.Bals R, Boyd J, Esposito S, Foronjy R, Hiemstra PS, Jiménez-Ruiz CA, et al. Electronic cigarettes: A task force report from the European Respiratory Society. The European Respiratory Journal. 2019;53(2):1801151
28.Veit T, Munker D, Leuschner G, Mümmler C, Sisic A, Kauke T, et al. High prevalence of falsely declaring nicotine abstinence in lung transplant candidates. PLoS One. 2020;15(6):e0234808
29.Mekov E, Ilieva V. Machine learning in lung transplantation: Where are we? Presse Médicale. 2022;51(4):104140
30.Barac Y, Silvestri SC, Daneshmand MA, Goldstein JD. Textbook of Transplantation and Mechanical Support for End-Stage Heart and Lung Transplantation. USA: John Wiley & Sons Ltd; 2024. p. 1037
31.Riddell P, Egan JJ. International donor conversion rates for lung transplantation need to be standardized. The Lancet Respiratory Medicine. 2015;3(12):909-911
32.Vos R, Patterson A, Raemdonck DV. In: LoCicero J III, Feins RH, Colson YL, Gaetano R, editors. Chapter 88, Shield’s General Thoracic Surgery. 8th ed. USA: Wolters Kluwer; 2019. pp. 1115-1143. Available from: https://lccn.loc.gov/2017051947
33.Van der Mark S, Hoek RAS, Hellemons ME. Developments in lung transplantation over the past decade. European Respiratory Review. 2020;29:190132. DOI: 10.1183/16000617.0132-2019
34.Aleyadeh W, Verna EC, Elbeshbeshy H, Sulkowski MS, Smith C, Darling J, et al. Outcomes of early vs late treatment initiation in solid organ transplantation from hepatitis C virus nucleic acid test-positive donors to hepatitis C virus-uninfected recipients: Results from the HCV-TARGET study. American Journal of Transplantation. 2024;24:468-478
35.Lemaitre PH, Tikkanen JM, Mariscal A, Singer LG, Keshavjee S. Lung transplantation. In: Darling GE, Baumgartner WA, Jacobs JP, editors. Pearson’s General Thoracic Surgery. USA: STS Cardiothoracic Surgery E-Book. STS 2021. Ebook.sts.org. The Society of Thoracic Surgeons. 2024. Available from: https://ebook.sts.org/sts/index/Pearsons-General-Thoracic/Thoracic; [Accessed: December 2023]
36.Krishnan P, Saddoughi SAD. Procurement of lungs from brain-death donors. Indian Journal of Thoracic and Cardiovscular Surgery. 2021;37(Suppl. 3):S416-S424. DOI: 10.1007-021-01140-1
37.Loor G, Shumway SJ, McCurry KR, et al. Process improvement in thoracic donor organ procurement: Implementation of a donor assessment checklist. Annals of Thoracic Surgery. 2016;102(6):1872-1877
38.Copeland H, Hayanga JWA, Neyrink A, et al. Donor Heart and Lung Procurement: A Consensus Statement. Elsevier Inc. on Behalf of International Society for Heart and Lung Transplantation. Jun 2020;39(6):501-517. DOI: 10.1016/j.healun.2020.03.020
39.Inci I. Donors after cardiocirculatory death. Journal of Thoracic Disease. 2017;9(8):2660-2669. DOI: 10.21037/jtd.2067.07.82
40.Date H. Current status and problems of lung transplantation in Japan. Journal of Thoracic Disease. 8 Aug 2016;(Suppl. 8):S631-S636. DOI: 10.21037/jtd.2016.06.38
41.Date H. Living-related lung transplantation. Journal of Thoracic Disease. 2017;9(9):3362-3371. DOI: 10.21037/jtd.2017.08.152
42.Nguyen DC, Loor G, Carrott P, Shafii A. Review of donor and recipient surgical procedures in lung transplantation. Journal of Thoracic Disease. 2019;11(Suppl. 14):S1810-S1816. DOI: 10.21037/jtd.2019.06.31
43.Yu WS, Son JA. Donor selection, management, and procurement for lung transplantation. Journal of Chest Surgery. 2022;55(4):277-282. DOI: 10.5090/jcs.22.068
44.Watanabe T, Cypel M, Keshavjee S. Ex vivo lung perfusion. Journal of Thoracic Disease. 2021;13(11):6602-6617. DOI: 10.21037/jtd-2021-23
45.Wauwer C, Suylen V, Zhang LZ, et al. Is logistically motivated ex vivo lung perfusion a good idea? Frontiers in Transplantation. 2022;1:12. DOI: 10.3389/frtra.2022.988950
46.Gust L, D’Journo XB, Briounde G, et al. Single-lung and double-lung transplantation: Techniques and tips. Journal of Thoracic Disease. 2018;104(4):2508-2518. DOI: 10.21037/jtd.2018.03.187
47.Park S, Kim YT. Technical aspects of lung transplantation: General considerations. Journal of Chest Surgery. 2022;55(4):301-306. Available from: https://orcid.org/0000-0001-9006-4881
48.Murala JS, Hanif HM, Peltz M, et al. Lung transplantation: How to do it. Indian Journal of Thoracic and Cardiovascular Surgery. 2021;37(Suppl. 3):S454-S475. DOI: 10.1007/s12055-021-01218-w
49.Date H. Living-donor lobar lung transplantation. The Annals of Thoracic Surgery. 2021;112:1055-1058. Available from: https://10.1016/j.athoracsurg.2021.06.0511
50.Suh JW. Surgical complications affecting the early and late survival rates after lung transplantation. Journal of Chest Surgery. 2022;55(4):332-337. Available from: https://orcid.org/0000-0003-0287-0651
51.Saeedan MB, Mukhopadhyay S, Lane CR, Renapurkar R. Imaging indications and findings of lung transplant draft dysfunction and rejection. Insights into Imaging. 2020;11:2. DOI: 10.1186/s13244-019-0822-7
52.Riley L, Lascano J. Clinical outcomes and survival following lung transplantation in patients with Alha-1 antitrypsin deficiency. Respiratory Medicine. 2020;172:106145. DOI: 10.1016/j.rmed.2020.106145
53.Greer M, Welte T. Chronic obstructive pulmonary disease and lung transplantation. Seminars in Respiratory and Critical Care Medicine. 2020. DOI: 10.1055/s-0040-1714250
54.Date H. Living-donor lung transplantation. The Journal of Heart and Lung Transplantation. Article in press. 2023. DOI: 10.j.healun.2023.09.006
55.Verleden GM, Gottlieb J. Lung transplantation for COPD and emphysema. European Respiratory Review. 2023;32:220116. DOI: 10.1183/16000617.0116-2022
56.Gulack BC, Mulvihill MS, Ganpathy AM, et al. Survival after lung transplantation in recipients with Alpha-1-antitrypsin deficiency compared of chronic obstructive pulmonary disease: A national cohort study. Transplant International. 2018;31(1):45-55. DOI: 10.1111/tri.13038
57.Weill D, Keshavjee S. Lung transplantation for emphysema: Two lungs or one. The Journal of Heart and Lung Transplantation. 2001;20:739-742
Written By
Alina Ligia Cornea, Seamus Linnane, Peter Riddell, Diana Parau and Alexandru Mihai Cornea
Submitted: 25 February 2024Reviewed: 26 February 2024Published: 02 May 2024